

Mental Health Impacts of Covid-19
Is it fear of contracting, grief for loved ones, or simply stress about the whole thing?

My loving partner sent me a Vox article yesterday and told me that it seemed like mental health strains during the pandemic were more tied to case counts than to lockdown measures. He loves to tell me reasons why I should get over my pandemic despair and this was a perfect little way to slip it into conversation. The article shows that rates of mental health distress (either anxiety or depression) have been moving in lockstep with case counts here in the US. Here’s my version of their chart:
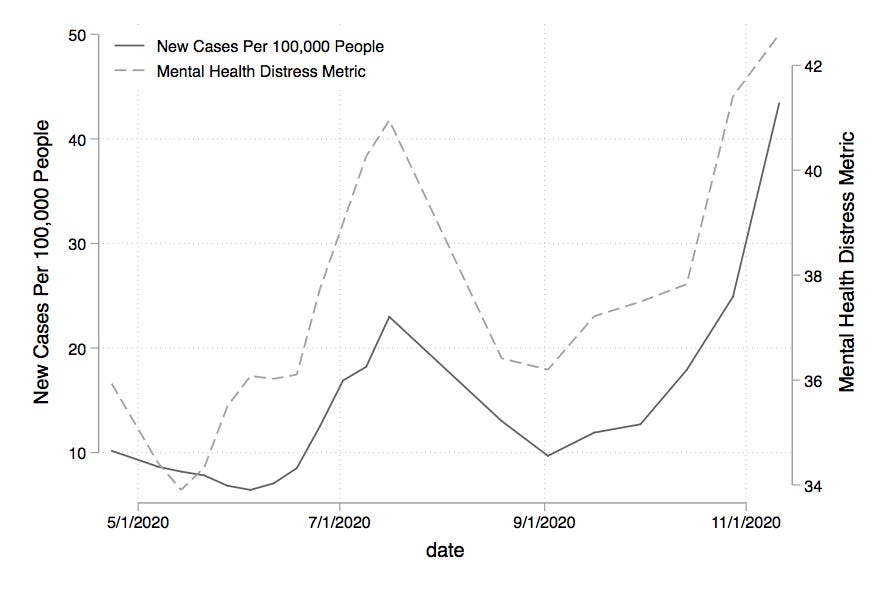
Pretty wild! That looks like a seriously strong correlation. But to the keen economist eye and the raging feminist heart, I knew the story didn’t end there and I was going to prove it. And look what I found!

This chart plots the state averages for the mental health distress metric over their average number of new cases per 100,000 residents over the sample dates. There is literally a negative correlation between the number of new cases and mental distress. North and South Dakota really stick out as having the highest average number of new cases per 100,000 (over the sample period) and also the lowest measures of mental health distress. If you plot mental health distress against the data on deaths by state, you get no correlation at all.
So what does this tell us? Well for starters, it tells us that it doesn’t appear to be the case that being in a place with higher rates of covid-19 makes people more likely to experience symptoms of depression and anxiety. Instead, the data indicate that the depression and anxiety people are facing is at least somewhat detached from real risk rates. People in California and Oregon have much lower risk of picking up the virus off of the street and yet report some of the highest rates of depression and anxiety symptoms. Of course, many people have loved ones who live in a different states, so grief could very well be contributing to the picture here. But still, one would think that grief en masse would be elevated in the locales where suffering and death were at their highest?
On the other hand, when case rates rise nationally, we do see an increase in national mental health distress. How is this possible? Could it be that mental health is more tied to economic security, or isolation? Seems to me that all of us in California - where case rates per 100,000 are relatively low but mental distress high - are just sitting and watching that New York Times chart update. And as we watch the country worsen, even if our state is doing relatively better, we see the length of lock-downs and the amount of national suffering rise and feel our own power in this battle dwindle ever smaller.
For those interested, I also ran a series of regressions to test the hypothesis that the correlation between cases and depression/anxiety is driven by the time series and not by region (i.e. local risk). In each specification I ran, I found that once time fixed effects were included in the regression, the strong positive relationship disappeared. For example, I’ve included some simple binned scatter plots with death growth rates plotted against depression and anxiety symptoms reported at the state-date level (with a frequency of approximately every two weeks, with some exceptions). Without any fixed effects, we see the strong positive relationship we’d expect.

But when we add a time fixed effect - basically taking the time trends I plotted in the first chart out of the data so that we’re looking primarily at the variation in cases and mental health across states - we get no relationship.

No matter what definitions I use - case counts, case growth rates, death counts, death growth rates, past rates, present rates - I get the same result. Mental health distress rises and falls with total national case counts, but is not correlated with regional intensity of virus spread or mortality. This gives us just a start for thinking about how and why the pandemic has impacted people’s mental health. And the picture is not as clear as one might hope.
I’ve uploaded my Stata code to Dropbox in case anyone wants to play around or check my work. Links to the data sources are included below. This is obviously not super sophisticated work, but feel free to send feedback or thoughts on how to think further about these issues!
Data sources:
1) Mental Health Data from the CDC - NCHS: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm
2) Covid case and death data from the New York Times: https://github.com/nytimes/covid-19-data/blob/master/us-states.csv
3) State populations from the US Census Bureau via Wikipedia: https://simple.wikipedia.org/wiki/List_of_U.S._states_by_population